
Treating milia at home is one of the most-searched skin questions of 2026, and for good reason: those tiny pearl-white bumps along the cheekbones and
Treating milia at home is one of the most-searched skin questions of 2026, and for good reason: those tiny pearl-white bumps along the cheekbones and under-eye area refuse to budge with normal cleansing. They are not pimples or whiteheads, and trying to squeeze them like a clogged pore usually leaves you with redness, broken capillaries, or a faint scar. This guide walks through what milia actually are, what causes the recent uptick, the gentle ingredient routine that gradually clears them, the mistakes that make things worse, and the cases when a dermatologist is the right call. Safety first throughout.
This guide was reviewed by the BeautynFacts editorial team. Last updated: June 2026.

A Quick Safety Note Before You Start
This is cosmetic skincare guidance, not medical advice. The routine below is for scattered milia that appear on otherwise healthy adult skin. If you have a dense cluster, milia in a child, milia that appeared after a burn or rash, or any bump that is changing color, growing, or painful, skip the home routine and see a dermatologist. Persistent milia en plaque (a raised plaque with multiple bumps), milia tied to an autoimmune condition, and milia in infants all need clinical evaluation. Nothing in this article replaces that visit.
What Milia Actually Are (and Why They Are Trending in 2026)
Milia are small keratin cysts. They form when dead skin cells (keratin) get trapped under the surface instead of shedding through a pore. The result is a firm, dome-shaped bump, usually 1 to 2 millimeters across, white or yellowish, most often on the cheekbones, under the eyes, around the nose, and on the forehead. Home treatment has become a bigger conversation in 2026 because the clean-girl and glass-skin trends sent everyone toward heavier balms, occlusive overnight masks, and rich eye creams, and a noticeable share of users picked up new bumps as a side effect.
Unlike a whitehead, a milium has no visible pore opening on top. That is the single most important fact about them, and it explains why squeezing or steaming does almost nothing.
The Numbers Behind the Milia Surge
Search interest for milia removal and related queries has climbed steadily through the first half of 2026, with the biggest jumps from users in their late twenties to mid-forties. Dermatology clinics report that the cosmetic consult for milia removal is now one of their most common five-minute appointments, especially after winter, when occlusive routines peak. On TikTok and Pinterest, before-and-after content tagged with milia keywords has crossed into the high tens of millions of cumulative views over the past year. The pattern echoes the closed-comedone wave of 2023: a slow-burn skin concern that gets louder as more people learn the correct name for what they are seeing.
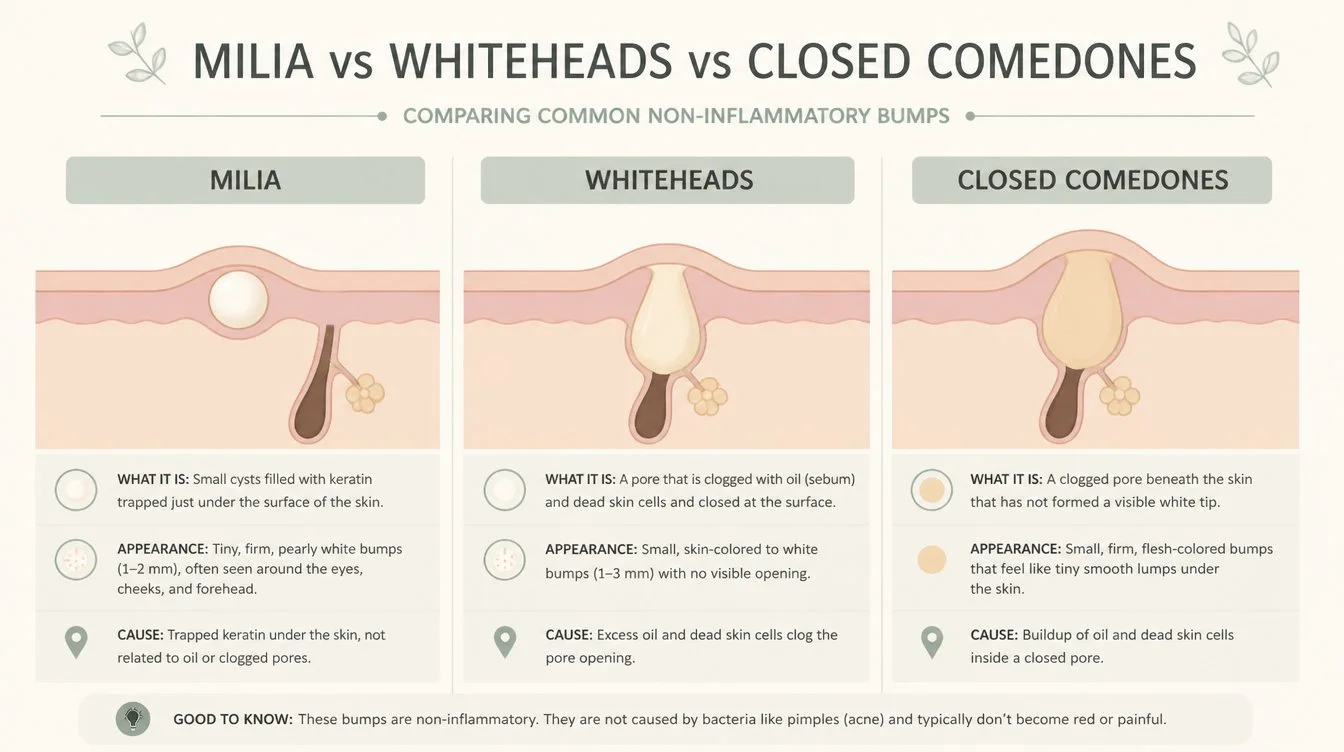
Milia vs Whiteheads vs Closed Comedones vs Syringomas
The confusion is constant, and it matters because the fix is different for each.
Milia are keratin cysts trapped under intact skin. They have no pore opening, feel firm, are often pearly white, and sit just under the surface. They do not respond to typical acne care.
Whiteheads are blocked pores with a visible opening. The contents are softer, the bump is rounder and less firm, and salicylic acid clears them relatively quickly.
Closed comedones are skin-colored bumps from clogged follicles, usually in clusters along the forehead, jaw, or hairline. They are softer than milia and respond to retinoids and BHA over weeks.
Syringomas are small benign growths from sweat glands, often yellow or skin-toned, frequently mistaken for milia on the lower eyelid. They do not respond to topicals at all and need a dermatologist for cosmetic removal.
If your bumps have been there for months, do not respond to any acid, and sit specifically on the lower eyelid in a soft cluster, consider that they might be syringomas rather than milia.
What Causes Milia (the Honest Answer)
Sometimes there is a clear trigger and sometimes there genuinely is not. The common causes:
Heavy creams and balms near the eye area. Rich textures rated for the cheek can be too occlusive for the delicate periocular skin, where the barrier sheds differently.
Heavy mineral sunscreens. Some thick, water-resistant zinc formulas, especially the tinted ones layered daily under makeup, are repeat offenders.
Sun damage. Years of UV exposure thicken the upper layer of the skin, slow natural exfoliation, and create conditions that trap keratin.
Trauma to the skin. Burns, blistering rashes, aggressive laser treatments, and even very harsh scrubs can trigger secondary milia weeks later.
Genetics. Some people simply form milia easily, the same way some people scar more visibly than others. There is nothing wrong with your routine if you fall into this group; it just means the maintenance plan takes time.
Nothing identifiable. Yes, really. Primary milia in healthy adult skin sometimes appear with no clear trigger, and that is documented.
Milia can show up on any skin tone or skin type. They are most common on the upper cheekbones, the under-eye area, the bridge of the nose, the forehead, and occasionally along the jawline. On medium and deep skin tones, they can look slightly yellow rather than bright white, which sometimes makes them harder to spot until a catchlight from a phone flash reveals the texture. Dry and combination skin types report them more often than oily skin types, but no group is immune.
How to Treat Milia at Home: The Gradual Clear Routine
The plan that works is unglamorous: gentle, consistent chemical exfoliation plus a retinoid, run for six to twelve weeks. Here is the step-by-step routine without irritating the surrounding skin.
- Audit the current routine first. Pull every product you use within four inches of the milia. Anything thicker than a light lotion, anything labeled balm, anything tagged as a sleeping pack or occlusive mask: pause it for the duration of treatment.
- Switch the cleanser to a gentle gel or cream cleanser. Twice daily. No grainy scrubs, no rough washcloths, no facial brushes during this period.
- Add a salicylic acid (BHA) step three nights a week. A 0.5 to 2 percent leave-on serum or toner, applied only to the bumpy areas after cleansing and before moisturizer. BHA is oil-soluble and can work its way into the keratin plug from above.
- Add a glycolic or lactic acid (AHA) step two mornings a week. Use a 5 to 8 percent AHA toner or serum, and layer sunscreen on top. AHAs lift the dead surface layer so the underlying bump is closer to the open air, which is how the body eventually clears the keratin out.
- Add a retinoid four nights a week. An over-the-counter retinol at 0.3 to 1 percent, or a prescription tretinoin 0.025 percent if you already have one. Apply a pea-sized amount over the full face on retinoid nights, including the bump zones. Skip the BHA on retinoid nights.
- Moisturise with a light, non-occlusive lotion. Look for words like “fluid,” “gel-cream,” or “light lotion” on the label. Avoid balm, butter, or rich cream textures near the bumps.
- Sunscreen every single morning. Use a fluid or light lotion with SPF 30 or higher. Heavy zinc sticks and thick water-resistant sport SPFs can be a trigger; save those for outdoor sport days.
- Patience. Most adult milia will start to flatten between weeks four and eight. Some take a full twelve weeks. Resist the urge to escalate the routine before the eight-week mark.
If you do only one thing from the list, do the salicylic acid plus a retinoid and run it for at least six weeks before judging the results.

The Dermatologist Version (and What It Costs)
When a clinician removes milia, the standard method is a single-use sterile lancet to make a tiny opening over the cyst, followed by gentle expression with a comedone extractor. The procedure takes about thirty seconds per bump in trained hands; the skin is closed within minutes, and the risk of scarring is very low because the depth and angle are controlled. For larger or deeper milia, the dermatologist may use light electrocautery or cryotherapy instead. A typical cosmetic milia removal session in 2026 runs roughly USD 100 to 300, or INR 2,500 to 8,000 depending on the city and the number of bumps treated. Many clinics include a same-week follow-up and topical recommendations in the price.
One thirty-minute appointment can clear a dozen visible bumps, which is why even committed home-routine users sometimes book a single session and then maintain the result with the at-home plan.
Variations of the Home Routine to Try in 2026
The minimalist is clear. A 2 percent salicylic acid leave-on three nights a week, light gel moisturizer, and fluid SPF in the morning. Best for sensitive skin that cannot tolerate retinoids yet.
The retinoid-led plan. A 0.5 to 1 percent retinol nightly after a four-week ramp, with one BHA night a week and one AHA morning a week. Best for tolerant skin.
The mandelic add-on. Mandelic acid (10 percent) is used as the AHA instead of glycolic. It has a larger molecule, which means slower penetration and less irritation. This product is effective for medium and deep skin tones that pigment easily.
The PHA is gentle daily. Polyhydroxy acids like gluconolactone are used as a daily toner. Slower clearing but very low irritation.
What NOT to Do at Home (the Safety Section)
This is the section that protects you from a permanent scar.
Do not pierce milia with a sewing needle, safety pin, or bobby pin. Even if you sterilize the tip with alcohol or a flame, the skin around your eyes is two to three times thinner than the skin on your cheek, the angle is hard to control with your own non-dominant hand, and the infection rate from non-clinical extraction is meaningfully high. The TikTok clips that show this technique are precisely the wrong thing to copy.
Do not pick at, scratch, or squeeze hard. Milia do not have pore openings. Pressing harder does not open a milia; it bruises the surrounding skin, which can become pigmented for weeks on medium and deep skin tones.
Do not steam the face in hopes of opening the bumps. Steam softens the skin temporarily but does not dissolve keratin and does not create a pore where none exists.
Do not stack acids on day one. A common mistake: people read a list like this one, then use BHA, AHA, and retinol all on the same first night. The barrier may flare, the milia may persist, and the surrounding skin may worsen. Introduce one new active ingredient each week.
Do not over-exfoliate with grainy scrubs or facial brushes. Physical exfoliation does not reach the cyst and does damage the surface. Chemical exfoliation is the right tool.
Do not apply retinoids or strong acids directly to the eyelid. Treat the bumps that are on the cheekbone, brow, and forehead area only. For milia on the lash line, you need to see a dermatologist.
Ingredients and Product Categories That Actually Work
You do not need a long shelf to clear them. Here is what to look for on labels.
Salicylic acid (BHA), 0.5 to 2 percent. Oil-soluble, it can penetrate the keratin. Look for it in leave-on serums and toners, not rinse-off cleansers.
Glycolic acid (AHA), 5 to 10 percent. The fastest-acting surface exfoliant. Look for formulas with a buffered low pH around 3.5 to 4 and a hydrating partner ingredient.
Lactic acid (AHA), 5 to 10 percent. A larger molecule than glycolic, it’s gentler, with mild hydration. Good first AHA for reactive skin.
Mandelic acid, 5 to 10 percent. Slowest penetration, lowest irritation rate. This option is the pick for melanin-rich skin.
Retinol or adapalene. A 0.3 to 1 percent stabilized retinol or an over-the-counter 0.1 percent adapalene speeds up the cell turnover cycle, which is the underlying mechanism that prevents keratin from getting trapped.
Niacinamide, 4 to 5 percent. Helps keep the surrounding barrier intact while the actives do their work.
What to avoid on the label: petrolatum-heavy balms, lanolin-rich creams, heavy mineral oil formulas, thick zinc sticks, and any sleeping mask labeled occlusive or barrier-sealing.
Home Routine vs In-Office Removal: How to Choose
Pick the at-home route if your milia are scattered (under ten visible bumps); have appeared in the last six months; are not on the lash line or lid margin; and you are willing to run a routine for two to three months. Choose the in-office route for a dense cluster (more than fifteen bumps in one zone); bumps that have been there for over a year and have not responded to acids and retinoids; bumps on the lower lash line; bumps in a child; or an event in under eight weeks that the home routine will not finish in time for. A reasonable middle path is one clinical removal session for the visible cluster, then the at-home routine as ongoing maintenance to prevent return. That combination is what many dermatology patients actually do in practice.
How Long the Clear Routine Takes (Realistic Timeline)
Weeks one to two: skin adjusts to the actives. Some early flaking is normal. Bumps look unchanged.
Weeks three to four: surrounding texture starts to look smoother. The bumps may read as slightly less raised.
Weeks five to eight: visible bumps start to flatten; some disappear entirely. New formation slows.
Weeks nine to twelve: the original cluster usually thins to a few stubborn holdouts that may need clinical removal. The maintenance routine takes over from active clearing.
If you have seen no change at all by week eight, that is the signal to either escalate the routine with caution or book a dermatologist for a single removal session.
Frequently Asked Questions About Milia at Home
Can you get rid of milia at home, or do you need a dermatologist?
You can clear most scattered, recent milia at home with a gentle routine of salicylic acid two or three nights a week, a low-strength retinoid four nights a week, an AHA toner one or two mornings a week, light moisturizer, and daily sunscreen. Allow six to twelve weeks. A dermatologist is the right choice for dense clusters, milia on the lash line, milia in a child, milia that have been present for years, or bumps that do not respond to acids and retinoids after eight weeks. Many people combine one clinical removal with the home maintenance routine afterward.
What is the fastest way to get rid of milia naturally?
There is no genuinely fast natural fix. The fastest safe at-home approach is a leave-on salicylic acid serum at 2 percent three nights a week, paired with a retinoid (retinol or adapalene) four nights a week, with otherwise minimal skincare and sunscreen every morning. Most adults see flattening between weeks four and eight. Steam, lemon juice, sugar scrubs, and DIY needle extraction are not safe shortcuts and frequently leave pigmentation or scars. The fastest clinical option is in-office extraction, which clears visible bumps in a single appointment.
Why am I suddenly getting milia under my eyes?
Sudden under-eye milia almost always trace back to a routine change in the past one to three months. The usual suspects: a new, richer eye cream; a heavier sleeping mask layered into the routine; a thick mineral sunscreen used daily; or a recent occlusive balm used overnight on the under-eye area. Aggressive new exfoliation that damaged the barrier can also trigger them indirectly. Sun damage that has built up over years sometimes shows up as a fresh cluster after a high-UV holiday. Less commonly, a trigger cannot be identified, and the bumps appear on otherwise unchanged skin.
Is it safe to pop a milia cyst with a needle at home?
No. Milia have no pore opening, the skin around the eye is unusually thin, and the angle is very hard to control with your hand. Even a sterilized needle carries a meaningful infection risk in non-clinical conditions and can leave a permanent pinpoint scar, a stretched pore, or post-inflammatory pigmentation that lasts months on medium and deep skin tones. The dermatologist procedure looks similar but uses a single-use sterile lancet at a controlled depth with the right angle and stabilization. If at-home treatment is not working, please book an in-office removal rather than attempting it yourself.
What ingredients can actually dissolve milia?
Nothing applied topically truly dissolves a milium in one step; the bump is keratin under intact skin, not a surface plug. What works is gradual: salicylic acid at 0.5 to 2 percent softens the keratin by penetrating the upper layers, AHAs (glycolic, lactic, or mandelic) at 5 to 10 percent strip the surface so the bump sits closer to open air, and a retinoid (retinol 0.3 to 1 percent or adapalene 0.1 percent) speeds up the cell turnover cycle so trapped keratin works its way out. Used together for six to twelve weeks, this routine flattens most adult milia.
How long does it take for milia to go away with home treatment?
Plan for six to twelve weeks of consistent routine before judging results. The first two weeks are an adjustment period, and you may not see any visible change. Between weeks three and four, surrounding texture improves. Between weeks five and eight, visible bumps start to flatten, and some disappear entirely. By week twelve, most scattered milia have cleared or thinned to a few stubborn holdouts that may need clinical removal. Should you not see any improvement by week eight, consider escalating your treatment or scheduling an appointment with a dermatologist. Milia that have been present for years usually require in-office extraction rather than just a home routine.
Related Articles
- Cystic Pimples on the Back: Causes and Treatment
- Spot Treatments: What Actually Works on Active Breakouts
- Red Light Therapy: The Skin Benefits Explained